Multiple myeloma is a neoplastic plasma cell disorder commonly seen in elderly adults, characterised by punched-out lytic skeletal lesions, renal impairment, hypercalcemia, and monoclonal immunoglobulin production.
Description
Multiple Myeloma (MM) is a clonal B-cell malignancy characterised by the uncontrolled proliferation of plasma cells within the bone marrow, leading to the overproduction of monoclonal (M) proteins.
Pathogenesis
Multiple myeloma is a haematologic malignancy characterised by the uncontrolled proliferation of clonal plasma cells within the bone marrow. The disease develops from a premalignant condition called monoclonal gammopathy of undetermined significance (MGUS) in which plasma cells produce an excess amount of a single immunoglobulin. The transformation of MGUS to MM is not fully understood but is associated with multiple genetic abnormalities and changes in the bone marrow microenvironment.
Multiple myeloma profoundly affects bone metabolism through two key mechanisms:
- Increased osteoclastic activity – Clonal plasma cells secrete osteoclast-activating factors (e.g., RANKL, IL-6, MIP-1α, TNF-α), leading to excessive bone resorption.
- Suppressed osteoblastic function – Myeloma cells produce inhibitors of bone formation, including DKK-1 and sclerostin, which block Wnt signalling, preventing osteoblast differentiation and activity.
This imbalance results in trabecular destruction, diffuse osteopenia, and lytic bone lesions, which are hallmarks of myeloma bone disease
By comparison, MGUS is asymptomatic and involves a low clonal plasma cell burden (<10%) within the bone marrow. Over time, a subset of MGUS cases progress to smouldering myeloma and, ultimately, to multiple myeloma, following a spectrum of increasing plasma cell proliferation, genetic instability, and bone marrow microenvironment alterations.
Unlike MGUS, multiple myeloma is defined by clonal plasma cell infiltration (>10%) and evidence of end-organ damage (CRAB criteria: hypercalcaemia, renal failure, anaemia, bone lesions).
Bone Disease in Multiple Myeloma
Bone involvement in multiple myeloma results from an imbalance between osteoclastic activation and osteoblastic suppression:
- Increased Osteoclastic Activity
- Plasma cells secrete osteoclast-activating factors (e.g., RANKL, IL-6, MIP-1α, TNF-α), leading to aggressive bone resorption.
- This causes punched-out lytic lesions, vertebral compression fractures, and hypercalcaemia.
- Suppressed Osteoblastic Function
- Myeloma cells produce DKK-1 and sclerostin, inhibiting Wnt signalling and preventing osteoblast differentiation.
- Unlike other lytic conditions, myeloma does not induce reactive osteosclerosis.
Epidemiology, Risk Factors & Associations
- Multiple myeloma represents 1% of all cancers and approximately 10% of all haematologic malignancies.
- It’s more common in older individuals (median age at diagnosis is 70 years), males, and is twice as common in the African American population.
- Risk factors include radiation exposure, chronic immune stimulation, obesity, and a family history of the disease.
Clinical Features
Presents with a wide range of symptoms and signs which are typically associated with the acronym CRAB: Calcium elevation, Renal dysfunction, Anaemia, and Bone lesions.
- Bone Pain: The most common presenting symptom. Often located in the back or chest, it can be due to bone lesions or fractures.
- Pathological Fractures: Occur due to weakened bone from lytic lesions, commonly involving the vertebral column, ribs, pelvis, and proximal femur.
- Hypercalcaemia: Related to osteoclastic bone resorption, leading to confusion, polyuria, polydipsia, constipation, and in severe cases, coma.
- Renal Dysfunction: Caused by hypercalcaemia, light chain deposition, dehydration, and use of nephrotoxic medications. Up to 50% of cases.
- Anaemia: Normocytic normochromic. Almost universal in multiple myeloma, contributing to fatigue, weakness and dyspnoea.
- Infections: Frequent due to impaired immunity from abnormal immunoglobulin production and hypogammaglobulinaemia.
- Neurological symptoms: May occur due to cord compression, peripheral neuropathy or hyperviscosity syndrome (headache, dizziness, visual disturbances, confusion, and seizures).
- Amyloidosis: Deposition of light chains in organs can lead to organ dysfunction, particularly in the heart, kidneys, liver, and nerves.
Complications
Common complications include bone fractures, spinal cord compression, renal failure, recurrent infections, and hyperviscosity syndrome.
Subtypes
The disease is typically classified based on the type of monoclonal protein produced: IgG (50% of cases), IgA (20% of cases), IgD (less than 2% of cases), and light chain myeloma (20% of cases).
Pathological Features
Morphology
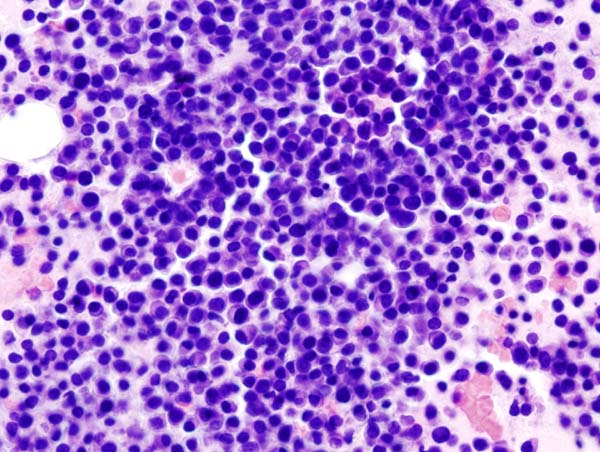
- Marrow Plasmacytosis: The bone marrow in myeloma is characterised by an excess of plasma cells, often forming aggregates or sheets.
- Plasma cells may show morphological variation, ranging from mature to immature forms, with occasional binucleate forms and ‘flame cells’.
- Red blood cells form a Rouleaux Formation
- Amyloid (AL subtype) deposits: In some cases, there can be systemic deposition of amyloid derived from the monoclonal light chains.
Histopathology
- The bone marrow biopsy shows a variable amount of plasma cells, usually more than 10% of all nucleated cells.
- These plasma cells often appear atypical, with an increased nucleus:cytoplasm ratio, and eccentrically placed nucleus.
- Bone damage: Bone biopsies will often show evidence of lytic lesions, with osteoclastic bone resorption due to increased production of RANKL by myeloma cells.
Biochemistry
- M-protein: 99% of patients have a monoclonal spike on serum protein electrophoresis (SPEP) and/or urine protein electrophoresis (UPEP). The M-protein is typically an IgG or IgA (less commonly IgD or IgE), or light chains only (Bence Jones proteins).
- Hypercalcemia: This may be present due to bone destruction.
- Renal insufficiency: Can occur due to light chain cast nephropathy, hypercalcemia, or amyloidosis.
- Anaemia: Normocytic normochromic. This is common due to bone marrow infiltration and decreased erythropoiesis.
- Beta-2 microglobulin: This is a subunit of the MHC class I molecule, and its levels correlate with the burden of disease.
Cytogenetics
- Various chromosomal abnormalities may be found in multiple myeloma, including translocations involving the immunoglobulin heavy chain locus (14q32) and deletions of chromosome 13 or 17p.
- The most common translocations involve oncogenes such as CCND1 (t(11;14)) and MMSET/FGFR3 (t(4;14)).
- These abnormalities can have prognostic significance.
Immunophenotyping
- Plasma cells in multiple myeloma are typically CD38 bright, CD138+, and CD56+, with monotypic cytoplasmic light chain restriction. They are usually negative for CD19 and CD45, which are typically expressed by normal plasma cells.
- Expression of CD20 can occur in a subset of cases and has been associated with t(11;14).
Radiological Features
General Features
Two common radiological appearances;
- Multiple, well-defined lytic bone lesions (punched-out appearance) without a sclerotic rim.
- Diffuse osteopaenia with vertebral compression fractures from osteoporosis
- Distribution identical to that of red marrow
- Frequent pathological fractures – vertebral bodies are destroyed before pedicles (vs. metastases in which pedicles are destroyed first).
- Extramedullary soft tissue masses in advanced disease.
- Raindrop skull: numerous small lytic skull lesions.
- Hair-on-end skull appearance due to extramedullary haematopoiesis in anaemia.
- Plasmacytoma tends to be large and expansile.
XR
- Punched-out lytic lesions, seen primarily in the skull, spine, ribs, pelvis, and proximal femur.
CT
- More precise assessment of bony destruction, fractures, osteolytic lesions, cortical breaches, and soft tissue masses.
MRI
MRI Patterns in Order of Increasing Severity
- Normal appearance (low tumour burden)
- Focal lesions – equal to or lower in signal intensity than muscle or disk on T1W images; hemorrhage into a lesion occasionally results in high signal equal to or lower in signal intensity than muscle or disk on T1W images; hemorrhage into a lesion occasionally results in high signal intensity in a focal lesion on T1W images. esions may be either low or high signal intensity in approximately equal numbers in untreated patient
- intensity in a focal lesion on T1W images
- Identical to metastases
- “Mini-brain” appearance – thick bone struts radiating inward from the outer margins of a focal lesion, resembling the sulci and gyri of the brain
- intensity in a focal lesion on T1W images
- Variegated (heterogeneous) – many small, low signal intensity foci on T1W images
- Diffuse (homogeneous) – homogeneous pattern of marrow replacement without features to distinguish it from many other marrow proliferative entities
- T1: Decreased signal intensity in affected bone marrow due to fat replacement.
- T2: Increased signal intensity due to elevated water content.
- Post-contrast: Varied enhancement patterns distinguish active from inactive disease.
- Preferred modality for suspected spinal cord compression.
PET/CT
- Increased FDG uptake in active myeloma lesions, beneficial for evaluating disease activity, treatment response, and extramedullary disease detection.
Grading and Staging
The Durie-Salmon system and the International Staging System (ISS) are used for staging. The ISS is preferred due to its simplicity and good correlation with prognosis, it’s based on beta-2 microglobulin and albumin levels.
Prognosis
Prognosis depends on the stage of disease, with a median survival of more than 5 years for stage 1 disease, but only 2 years for stage 3 disease.
Differential Diagnosis
- Monoclonal Gammopathy of Undetermined Significance (MGUS): This is a precursor condition with a monoclonal protein present, but without symptoms or findings seen in multiple myeloma. Differentiated by lower levels of M protein, absence of lytic lesions and normal plasma cell count in the bone marrow.
- Smouldering Multiple Myeloma (SMM): Also a precursor to myeloma, but with higher levels of M protein and more plasma cells in the bone marrow. However, it does not have the end-organ damage seen in myeloma. 75% progress to multiple myeloma within 15 years.
- Solitary Plasmacytoma: This is a single isolated lesion of clonal plasma cells, either in bone or soft tissue. Absence of systemic symptoms or other myeloma criteria differentiates it from multiple myeloma.
- Lymphoma: May also cause bone lesions and a high serum protein level, but typically it has a different pattern on bone marrow biopsy, lymphadenopathy on imaging, and presence of lymphoma cells rather than plasma cells. Non-Hodgkin lymphoma commonly demonstrates a moth-eaten or permeative pattern of bone destruction.
- Metastatic disease: Rarely involves intervertebral disc and mandible (c.f. MM), commonly affects vertebral pedicles (c.f. MM), not usually associated with large soft tissue mass (c.f. MM). Osteolytic lesions may originate from thyroid and renal malignancy.
- Primary Hyperparathyroidism: This can cause hypercalcemia and bone disease, but PTH levels are elevated, unlike in multiple myeloma.
- Amyloidosis: Can be associated with myeloma but may also occur independently. Differentiated by the systemic deposition of amyloid protein and specific organ involvement.
Management
Initial steps involve confirming the diagnosis with a bone marrow biopsy, serum protein electrophoresis, and imaging to assess the extent of the disease. Treatment typically involves chemotherapy, autologous stem cell transplantation in eligible patients, and supportive measures such as bisphosphonates for bone disease. The management usually requires a multidisciplinary team including haematologists, radiologists, and pathologists.