Liver
Description
The liver, the largest gland in the human body, weighs approximately three pounds in an adult and serves as one of the body’s most vital organs. Beyond its role as an accessory digestive organ, the liver performs essential metabolic and regulatory functions, including detoxification, bile production, and the processing of nutrients. It is located in the right upper quadrant (RUQ) of the abdominal cavity, just beneath the diaphragm, and is partially protected by the overlying ribs.
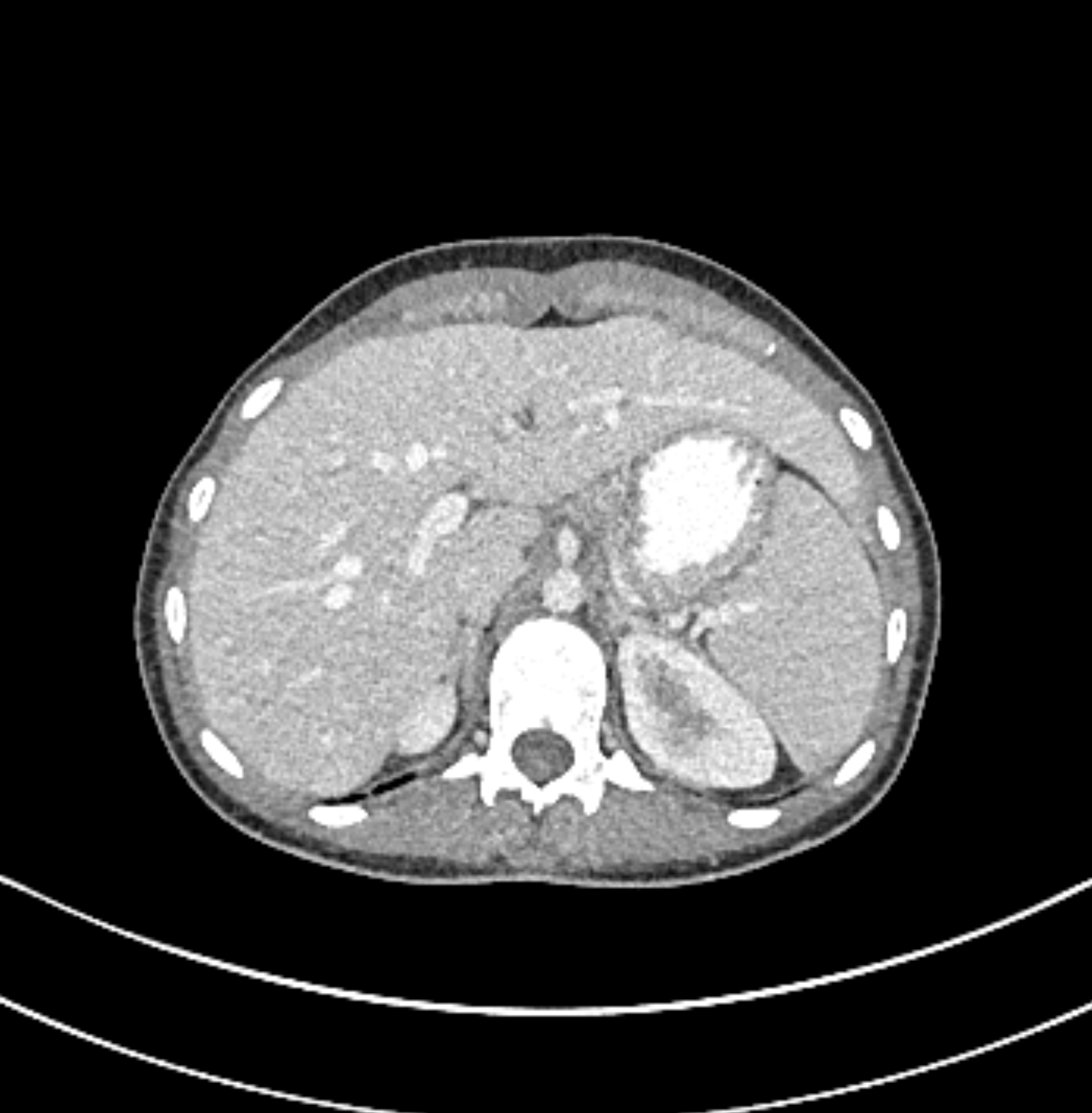
[image_scroll folder_url=”https://radiologica.org/wp-content/uploads/imaging-studies/ax_art_jpeg” total_images=”19″ start_index=”2″]
The liver’s hilum, known as the porta hepatis, serves as the entry and exit point for key structures, including the hepatic artery, hepatic portal vein, and the common hepatic duct. These structures travel along the lateral edge of the lesser omentum before reaching their destinations within the liver. The hepatic artery delivers oxygen-rich blood from the heart, while the hepatic portal vein carries nutrient-rich but partially deoxygenated blood from the gastrointestinal tract. Interestingly, the hepatic portal vein supplies more oxygen to the liver than the smaller hepatic arteries, due to the larger volume of blood it carries. This portal blood also contains absorbed drugs and toxins for processing.
Once inside the liver, blood is filtered through the hepatic sinusoids, where nutrients and toxins are metabolized. Processed blood flows into the central veins of each hepatic lobule, then drains into the hepatic veins, which ultimately empty into the inferior vena cava (IVC). This process, known as hepatic portal circulation, ensures that all blood from the gastrointestinal tract is filtered through the liver before reaching systemic circulation. This unique circulatory system is a key reason why the liver is a common site for metastases of cancers originating in the alimentary canal.
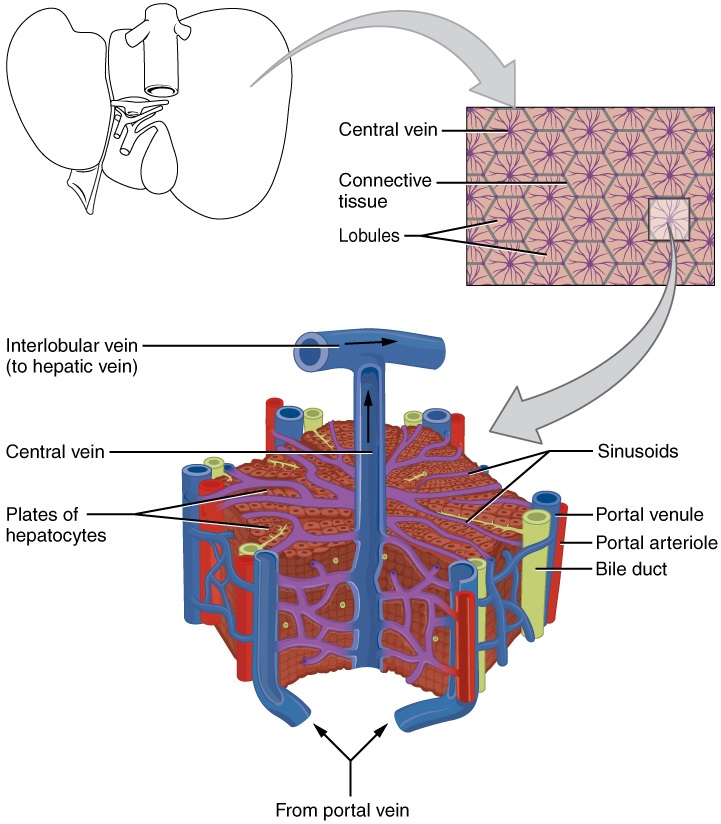
Microscopic Anatomy
The liver is a highly organised organ with three main microscopic components: hepatocytes, bile canaliculi, and hepatic sinusoids. Together, these structures form the foundation of the liver’s complex functions, including metabolism, detoxification, protein synthesis, and bile production.
Hepatocytes
Hepatocytes are the primary functional cells of the liver, constituting approximately 80% of the liver’s volume. These epithelial cells are polygonal in shape and arranged in plates or cords known as hepatic laminae, which radiate outward from the central vein in each hepatic lobule.
- Structure:
- Hepatocytes are packed with organelles such as mitochondria (for energy metabolism), rough and smooth endoplasmic reticulum (for protein and lipid synthesis), and peroxisomes (for detoxification).
- They have a high metabolic rate and are responsible for numerous biochemical activities, including glycogen storage, cholesterol synthesis, and drug detoxification.
- Functions:
- Secretory: Produce bile, which is essential for fat digestion and absorption.
- Endocrine: Release plasma proteins (e.g., albumin, clotting factors) and hormones into the blood.
- Metabolic: Process nutrients, toxins, and waste products carried by blood from the gastrointestinal tract.
Bile Canaliculi
Bile canaliculi are small, narrow grooves between adjacent hepatocytes that function as the initial ducts for bile collection.
- Formation and Flow:
- The grooves formed by adjacent hepatocyte membranes create canaliculi into which bile is secreted. Tight junctions between hepatocytes prevent bile leakage.
- Bile flows through the canaliculi into bile ductules, which eventually drain into larger bile ducts in the portal triad.
- The bile ducts unite to form the right and left hepatic ducts, which exit the liver as the common hepatic duct. The common hepatic duct merges with the cystic duct from the gallbladder to form the common bile duct, which delivers bile to the small intestine for digestion.
Hepatic Sinusoids
Hepatic sinusoids are specialised, porous capillaries that run between the hepatic laminae. These sinusoids bring oxygen-rich blood from the hepatic artery and nutrient-rich blood from the portal vein into close contact with hepatocytes.
- Structure:
- Sinusoids are lined by a fenestrated endothelium, which lacks a basement membrane, allowing for efficient exchange of nutrients, oxygen, and metabolites between hepatocytes and blood.
- The narrow space between sinusoidal endothelium and hepatocytes is known as the space of Disse, where exchange occurs.
- Blood Flow:
- Blood from the portal vein and hepatic artery flows through the sinusoids toward the central vein of each lobule.
- The central veins merge into larger hepatic veins, which ultimately drain into the inferior vena cava.
Kupffer Cells
Kupffer cells are star-shaped macrophages located within the hepatic sinusoids.
- Functions:
- Phagocytose dead red and white blood cells, bacteria, and foreign particles from blood flowing through the sinusoids.
- Play a role in immune surveillance and the clearance of endotoxins and debris from the bloodstream.
Portal Triad
At the periphery of each hepatic lobule is the portal triad, a characteristic arrangement of three major structures:
- Hepatic Artery Branch: Supplies oxygenated blood to hepatocytes.
- Hepatic Portal Vein Branch: Brings nutrient-rich but oxygen-poor blood from the gastrointestinal tract.
- Bile Duct: Collects bile produced by hepatocytes and transports it toward the small intestine.
These structures are surrounded by connective tissue and are connected to hepatocytes by sinusoids and bile canaliculi.
Functional Organisation
Blood and Bile Flow
One of the key aspects of liver organisation is the opposite flow of blood and bile:
- Blood Flow: From the portal triad through the sinusoids to the central vein, ultimately draining into the hepatic veins and the inferior vena cava.
- Bile Flow: From hepatocytes into bile canaliculi, then to bile ductules, bile ducts, and finally the common bile duct for secretion into the small intestine.
This countercurrent arrangement ensures that hepatocytes are exposed to both bloodborne nutrients and toxins for efficient processing while simultaneously producing bile for excretion.
Portal venous gas vs. pneumobilia
Pneumobilia is typically seen as linear branching gas within the liver most prominent in central large calibre ducts as the flow of bile pushes gas toward the hilum. This is in contrast to portal venous gas where peripheral small calibre branching gas is usually seen due to the hepatopetal flow of blood away from the hilum.




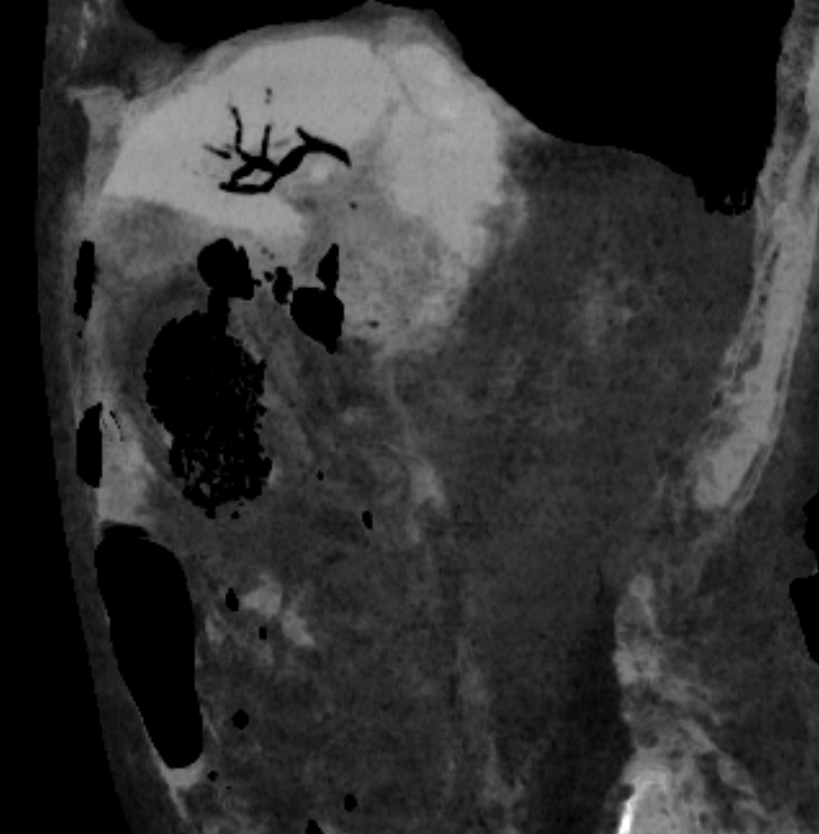
What is minIP? Learn more about image reconstruction in our Medical Imaging Physics Course!
Location
The liver is located in the right upper quadrant (RUQ) of the abdominal cavity, beneath the diaphragm. It primarily occupies the right hypochondrium and epigastric region, extending into the left hypochondrium.
Relational Anatomy
- Anterior: Anterior abdominal wall, diaphragm.
- Posterior: Diaphragm, inferior vena cava (IVC), right kidney, adrenal gland, and duodenum.
- Inferior: Gallbladder, stomach, duodenum, and transverse colon.
- Superior: Diaphragm, separating the liver from the pleura, lungs, heart, and pericardium.
- Lateral: Right hemidiaphragm, right kidney.
- Medial: Esophagus, stomach, and lesser omentum.
- Deep: The hepatic vessels and biliary system.
- Superficial: The Glisson’s capsule, a fibrous capsule surrounding the liver.
Development
The liver develops from the hepatic diverticulum, an endodermal outgrowth of the foregut, during the fourth week of embryogenesis. The hepatic cords form the parenchyma, while mesenchyme contributes to connective tissue and blood vessels. The biliary system originates from the same diverticulum, forming intrahepatic and extrahepatic bile ducts [2].
Function
- Bile secretion: Emulsifies fats for digestion and absorption in the small intestine.
- Detoxification: Removes toxins, drugs, and metabolic waste products.
- Metabolism: Processes carbohydrates, proteins, and lipids.
- Synthesis: Produces albumin, clotting factors, and other plasma proteins.
- Storage: Stores glycogen, vitamins (A, D, E, K, and B12), and iron.
- Immunological function: Houses Kupffer cells, which are macrophages involved in innate immunity.
Structure
The liver is divided into two anatomical lobes (right and left) and two smaller accessory lobes (caudate and quadrate) based on surface anatomy. Functionally, it is divided into eight segments (Couinaud classification) based on vascular supply and biliary drainage.
Anatomically, the liver is divided into two primary lobes: the larger right lobe and the smaller left lobe. Within the right lobe, two additional regions are often identified—the quadrate lobe (located inferiorly) and the caudate lobe (located posteriorly). These lobes are distinguished by internal structures, such as vascular and biliary landmarks. The liver is anchored to the diaphragm and abdominal wall by five peritoneal folds known as ligaments: the falciform ligament, the coronary ligament, two lateral ligaments, and the ligamentum teres hepatis. The falciform ligament and ligamentum teres hepatis are remnants of the embryological umbilical vein and demarcate the right and left lobes anteriorly. Additionally, the lesser omentum connects the liver to the lesser curvature of the stomach.
The Couinaud system divides the liver into four vertically-oriented sections (right posterior, right anterior, left medial, and left lateral) based on the three main hepatic veins, which act as boundaries. Horizontal division is achieved by the portal vein bifurcation, creating superior and inferior segments. These segments are numbered I to VIII, starting with the caudate lobe and proceeding in a clockwise direction.
Segment Definitions
- Segment I (Caudate Lobe):
- Independent of the portal venous branches and hepatic veins, with its own blood supply from both the right and left portal veins and hepatic arteries.
- Located posteriorly, it lies between the inferior vena cava (IVC) and the ligamentum venosum.
- Drains directly into the IVC, bypassing the hepatic veins.
- Segment II (Superior Left Lateral Segment):
- Located in the superior portion of the left lobe, lateral to the left hepatic vein.
- Supplied by the left portal vein.
- Segment III (Inferior Left Lateral Segment):
- Lies in the inferior portion of the left lobe, lateral to the left hepatic vein.
- Supplied by the left portal vein.
- Segment IV (Left Medial Segment):
- Divided into IVa (superior) and IVb (inferior).
- Located between the left hepatic vein and the middle hepatic vein.
- Supplied by the left portal vein.
- Segment V (Inferior Right Anterior Segment):
- Lies in the inferior portion of the right lobe, anterior to the right hepatic vein.
- Supplied by the right portal vein.
- Segment VI (Inferior Right Posterior Segment):
- Located inferiorly in the right lobe, posterior to the right hepatic vein.
- Supplied by the right portal vein.
- Segment VII (Superior Right Posterior Segment):
- Positioned superiorly in the right lobe, posterior to the right hepatic vein.
- Supplied by the right portal vein.
- Segment VIII (Superior Right Anterior Segment):
- Located superiorly in the right lobe, anterior to the right hepatic vein.
- Supplied by the right portal vein.
Key Radiological Landmarks for Segmentation
- Hepatic Veins:
- The three main hepatic veins (right, middle, and left) form vertical boundaries:
- Right Hepatic Vein: Divides the right lobe into anterior (V and VIII) and posterior (VI and VII) sections.
- Middle Hepatic Vein: Separates the right lobe from the left lobe.
- Left Hepatic Vein: Divides the left lobe into medial (IV) and lateral (II and III) segments.
- The three main hepatic veins (right, middle, and left) form vertical boundaries:
- Portal Vein:
- The horizontal plane of the portal vein divides the liver into superior (II, IVa, VII, VIII) and inferior (III, IVb, V, VI) segments.
- Ligamentum Teres and Ligamentum Venosum:
- These structures delineate the boundaries of the left lobe, specifically segment IV from segments II and III.
- Inferior Vena Cava (IVC):
- Marks the posterior margin of the liver and is adjacent to segment I (caudate lobe).
Radiological Imaging of the Couinaud System
Ultrasound (US)
- Segment Identification:
- Hepatic and portal veins are used as landmarks for dividing segments.
- Portal veins are echogenic due to their thick walls, aiding in visualization.
- Doppler imaging evaluates blood flow in the portal vein and hepatic veins, assisting in segmental mapping during interventional procedures.
Computed Tomography (CT)
- Pre-Contrast Imaging: Identifies the gross anatomy of the liver and adjacent structures.
- Contrast-Enhanced Imaging:
- Portal Venous Phase (60–70 seconds): Enhances the portal vein and allows for clear delineation of liver segments.
- Arterial Phase: Highlights vascular landmarks like hepatic arteries, aiding in segmental localization.
- Segment Localization:
- Portal veins are used to separate superior and inferior segments, while hepatic veins are used to demarcate vertical divisions.
Magnetic Resonance Imaging (MRI)
- T1-Weighted Imaging: Highlights vascular structures for segmental division.
- Post-Gadolinium Sequences:
- Dynamic imaging shows blood flow through hepatic arteries and portal veins.
- Hepatobiliary phase with gadoxetate disodium (Eovist) enhances functional hepatocytes, helping segmental localization.
- MRCP (Magnetic Resonance Cholangiopancreatography): Visualizes intrahepatic bile ducts, correlating them with segmental anatomy for biliary interventions.
Applications in Interventions
- Liver Resection: The Couinaud system guides segment-specific resections while preserving unaffected portions of the liver.
- Tumor Localization: Facilitates precise identification of lesions relative to segmental anatomy for surgery, biopsy, or ablative therapy.
- Transplantation: Critical for dividing donor livers for transplantation (e.g., left lobe or right lobe grafts).
Clinical Relevance
- Functional Segmentation: Each segment functions independently with its own vascular and biliary supply.
- Surgical Relevance: Enables surgeons to perform precise liver resections, sparing unaffected liver segments.
- Interventional Precision: Assists radiologists and oncologists in targeting specific regions for treatment (e.g., embolisation or ablation).
- Radiological Appearance:
- Ultrasound: Homogeneous echotexture with a hypoechoic or isoechoic appearance relative to the renal cortex. The portal veins have echogenic walls due to surrounding fibrofatty tissue.
- CT: On unenhanced CT, the liver has a slightly higher attenuation than surrounding soft tissues (40–60 HU). After contrast, the portal venous phase (60–70 seconds) is best for parenchymal evaluation.
- MRI: The liver has a homogenous intermediate signal on T1-weighted images and a higher signal on T2-weighted images. Gadolinium-enhanced sequences highlight vascular and lesion characteristics.
- Contrast Characteristics: Arterial phase enhancement is useful for detecting hypervascular lesions, while the portal venous phase is ideal for evaluating most parenchymal abnormalities.
- Normal Dimensions: The craniocaudal height of the right lobe is approximately 15–17 cm, and the thickness of the left lobe is 6–8 cm [3].
Arterial Supply
The liver is supplied by the dual blood supply of:
- Hepatic artery (25%): Branches from the common hepatic artery (celiac trunk).
- Portal vein (75%): Supplies nutrient-rich blood from the gastrointestinal tract.
Hepatic Artery
The hepatic artery delivers approximately 25% of the liver’s total blood flow, but it contributes 50% of the liver’s oxygen supply, as it carries highly oxygenated arterial blood from the systemic circulation. It arises as part of the celiac trunk, one of the three main branches of the abdominal aorta.
Pathway and Branching
- Coeliac Trunk:
- The hepatic artery originates from the coeliac trunk, which arises at the level of T12 or L1 from the abdominal aorta.
- Common Hepatic Artery:
- The coeliac trunk gives rise to the common hepatic artery, which courses to the right and branches into:
- Proper Hepatic Artery: Ascends along the hepatoduodenal ligament within the lesser omentum to the porta hepatis, providing blood to the liver.
- Gastroduodenal Artery: Supplies the stomach and duodenum.
- The coeliac trunk gives rise to the common hepatic artery, which courses to the right and branches into:
- Proper Hepatic Artery:
- The proper hepatic artery runs alongside the portal vein and bile duct (together forming the portal triad) in the hepatoduodenal ligament.
- It divides at the porta hepatis into the right hepatic artery and left hepatic artery, which supply the respective lobes of the liver.
- Right Hepatic Artery:
- Provides oxygenated blood to the right lobe of the liver and frequently gives off the cystic artery to the gallbladder.
- Left Hepatic Artery:
- Supplies the left lobe, the quadrate lobe, and parts of the caudate lobe.

Variant Anatomy of the Hepatic Arteries
Hepatic arterial anatomy is highly variable, and understanding these variations is critical, especially for hepatobiliary surgery, transplantation, and interventional radiology. The most common variations include:
- Replaced Right Hepatic Artery: Arises from the superior mesenteric artery instead of the proper hepatic artery.
- Replaced Left Hepatic Artery: Arises from the left gastric artery.
- Accessory Arteries: Additional arterial supply from aberrant branches of other vessels, such as the superior mesenteric or left gastric artery.
Portal Vein (75% of Total Blood Supply)
The portal vein supplies 75% of the total blood flow to the liver but only provides about 50% of the oxygen supply due to its lower oxygen content. This nutrient-rich blood is derived from the gastrointestinal tract, spleen, pancreas, and gallbladder, making the portal vein essential for processing absorbed nutrients, drugs, and toxins.
Pathway of the Portal Vein
- Formation:
- The portal vein is formed by the union of the superior mesenteric vein (SMV) and splenic vein posterior to the neck of the pancreas at the level of L2.
- The inferior mesenteric vein (IMV) typically drains into the splenic vein before its convergence with the SMV.
- Course:
- After formation, the portal vein ascends obliquely behind the pancreas and runs within the hepatoduodenal ligament alongside the hepatic artery and common bile duct.
- At the porta hepatis, it bifurcates into:
- Right Portal Vein: Supplies the right lobe and branches into anterior and posterior divisions.
- Left Portal Vein: Supplies the left lobe, caudate lobe, and quadrate lobe.
Segmental Blood Flow
The bifurcation of the portal vein ensures a segmental distribution of blood supply:
- Right Portal Vein:
- Divides into anterior and posterior branches, which supply segments V, VI, VII, and VIII (according to the Couinaud classification).
- Left Portal Vein:
- Divides into medial and lateral branches, which supply segments II, III, and IV, as well as part of the caudate lobe.
Portal Blood Composition
- The portal vein carries blood rich in:
- Nutrients: Glucose, amino acids, and lipids absorbed from the intestines.
- Toxins: Drugs, alcohol, and other harmful substances for detoxification.
- Hormones: Insulin and glucagon from the pancreas.
Clinical Relevance of Portal Blood Flow
- Portal Hypertension:
- Elevated pressure in the portal vein can lead to complications like varices, splenomegaly, and ascites.
- Liver Metastases:
- Cancers from the gastrointestinal tract frequently metastasize to the liver because portal blood delivers tumor cells directly to the liver.
Integration of Dual Blood Supply
The hepatic artery and portal vein converge at the porta hepatis and branch in parallel to supply the liver’s microvascular system, the hepatic sinusoids. Blood from both sources mixes within the sinusoids, ensuring the hepatocytes receive oxygen and nutrients simultaneously.
Unique Characteristics of Dual Blood Supply
- Oxygen Balance:
- Although the hepatic artery contributes less blood flow, it provides 50% of the liver’s oxygen.
- This dual supply ensures the liver remains functional even if one source is compromised.
- Nutrient Delivery:
- Portal vein blood provides the nutrients and substrates for metabolism.
- Adaptability:
- During times of reduced portal vein flow (e.g., during fasting or portal vein thrombosis), the hepatic artery compensates to maintain oxygenation.
Radiological Assessment of the Arterial Supply
Ultrasound (US)
- Doppler Ultrasound:
- Assesses flow velocities in the hepatic artery and portal vein.
- Normal portal vein flow is hepatopetal (toward the liver) with a velocity of 20–40 cm/s.
- Hepatic artery flow is low-resistance with continuous diastolic flow, reflecting the liver’s high oxygen demand.
Computed Tomography (CT)
- CT Angiography (CTA):
- Visualizes hepatic arterial anatomy and variants.
- Portal venous phase imaging (60–70 seconds post-contrast) highlights the portal vein and its branches.
Magnetic Resonance Imaging (MRI)
- MR Angiography (MRA):
- Non-invasive imaging of hepatic arteries and portal veins without ionizing radiation.
- Particularly useful for assessing hepatic arterial variants and portal vein thrombosis.
Digital Subtraction Angiography (DSA)
- Gold standard for hepatic arterial mapping, often performed before liver transplantation or interventional procedures.
Clinical Implications of the Arterial Supply
- Transarterial Therapies: Treatments such as transarterial chemoembolization (TACE) for hepatocellular carcinoma rely on the selective delivery of chemotherapeutic agents via the hepatic artery.
- Liver Transplantation: Arterial variations must be carefully mapped preoperatively to ensure successful anastomosis during transplantation.
- Portal Vein Obstruction: Conditions such as portal vein thrombosis necessitate compensation by the hepatic artery to sustain liver function.
Venous Drainage
The hepatic veins (right, middle, and left) drain the liver into the inferior vena cava (IVC) [4].
Lymphatic Drainage
The lymphatic drainage of the liver flows into the hepatic lymph nodes, which drain into the celiac lymph nodes and eventually the thoracic duct.
Innervation
- Sympathetic: Celiac plexus.
- Parasympathetic: Vagus nerve.
- Sensory: Phrenic nerve (Glisson’s capsule).
Normal Variants
Reidel’s lobe: A downward projection of the right lobe. hepatomegaly, the entire liver would be enlarged and displace intra-abdominal organs. has a sharp tip usually with normal angles between the anterior and posterior surfaces about 45–70°

Beaver tail: A downward projection of the right lobe. hepatomegaly, the entire liver would be enlarged and displace intra-abdominal organs.
- Accessory fissures: Additional grooves or fissures on the liver surface.
- Aberrant hepatic arteries: Commonly replaced right hepatic artery arising from the superior mesenteric artery.
Common Pathologies
- Cirrhosis: Chronic liver disease leading to fibrosis and architectural distortion.
- Hepatocellular carcinoma: Primary malignant tumor of the liver.
- Hepatic steatosis (fatty liver disease): Accumulation of fat within hepatocytes.
References
- Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 7th ed. Lippincott Williams & Wilkins; 2013.
- Sadler TW. Langman’s Medical Embryology. 13th ed. Wolters Kluwer; 2015.
- Siegel A, Sapra A. “Anatomy, Abdomen and Pelvis, Liver”. StatPearls Publishing; 2024.
- Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 41st ed. Elsevier; 2016.