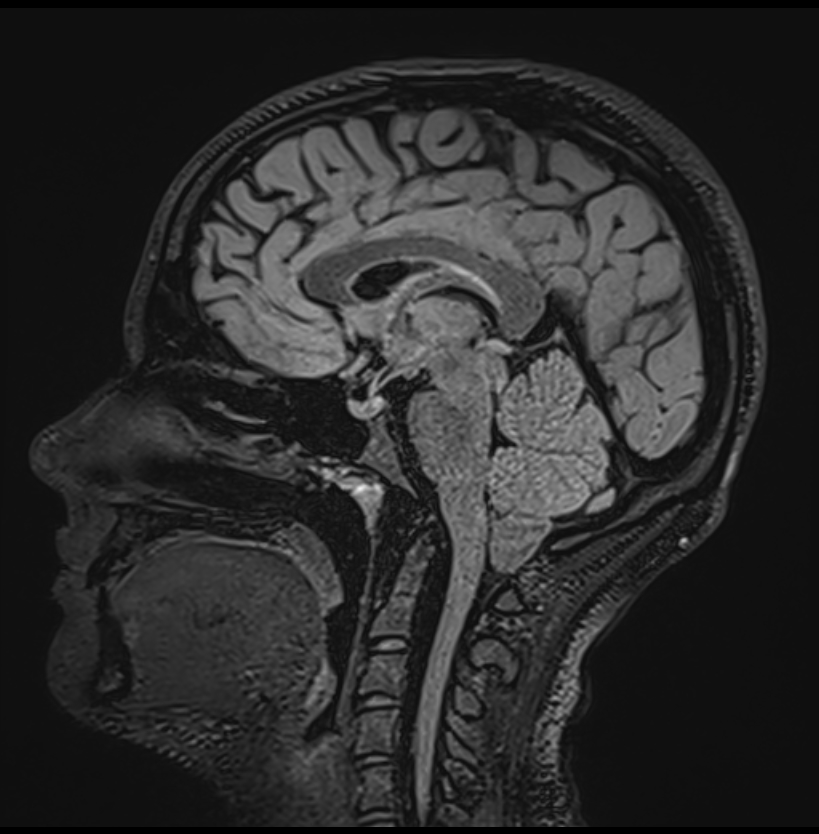
Chiari 1 Malformation is characterised by a caudal descent of the cerebellar tonsils through the foramen magnum.
Description
Chiari I Malformation is a congenital anomaly of the cerebellum characterised by a downward displacement of one or both cerebellar tonsils through the foramen magnum into the cervical spinal canal. It is the most common type of Chiari malformations, a group of complex congenital anomalies of the cerebellum.
Pathogenesis
The exact pathogenesis of Chiari 1 Malformation is not fully understood. However, it is thought to be due to a mismatch between the size of the posterior fossa and the volume of the cerebellum, leading to crowding at the foramen magnum and subsequent displacement of the cerebellar tonsils.
Epidemiology, Risk Factors & Associations
- Most commonly diagnosed in adolescence or adulthood (average age at diagnosis 25-40 years)
- Female preponderance (3:1 ratio)
Asssociations:
- Commonly associated with syringomyelia (30-70% of cases)
- Klippel-Feil anomaly (10%): fusion of 2 or more cervical vertebrae
- Basilar invagination (30%)
- Atlantooccipital fusion (uncommon)
- Not associated with Chiari II malformation
Clinical Features
- Often asymptomatic, detected incidentally on imaging for unrelated conditions
- Intermittent compression of brainstem:
- Nerve palsies
- Atypical facial pain
- Respiratory depression
- Long tract signs
- When symptoms occur, they may include headaches (often triggered by coughing, sneezing or straining), neck pain, dizziness, balance problems, and muscle weakness
Complications
- Potential for development of syringomyelia or hydrocephalus
- Rarely, severe brain stem compression and sudden death
Pathological Features
Histopathology
- Macroscopic: Caudally displaced cerebellar tonsils
- Microscopic: No specific microscopic changes in the cerebellar tissue
Radiological Features
General Features
- Characteristically demonstrates caudal descent of the cerebellar tonsils
- Adult: > 5mm below the McRae line
- Children: > 6mm below the McRae line
- McRae line – line drawn on a lateral radiograph of the skull or on a sagittal image from a CT or MRI scan that connects the posterior (opisthion) and anterior (basion) aspects of the foramen magnum.
- Descent between 3 – 5 mm is termed cerebellar ectopia
- Cerebella tonsils are pointed (rather than rounded).
- Syringomyelia (syrinx)
- The 4th ventricle may be elongated but remains in normal position
CT
- Non-contrast: May demonstrate low-lying cerebellar tonsils but MRI is more sensitive and specific
MRI
- T1WI: Low-lying pointed cerebellar tonsils >5mm below the foramen magnum in adults
- T2WI: May demonstrate associated syringomyelia (cavitary lesion within cord parenchyma, adjacent to central canal). Hypointense intralesional pulsation artefact may be present.
- T1 C+: No enhancement of the displaced cerebellar tonsils
Grading and Staging
No specific grading or staging system.
Diagnosis
Diagnosis is typically made based on MRI findings of caudal descent of the cerebellar tonsils, usually >5mm below the foramen magnum in adults.
Differential Diagnosis
- Tonsillar ectopia: Normal variant, inferior descent of tonsils <5 mm
- Chiari II malformation:Small posterior fossa with descent of the cerebellar vermis, rather than the tonsils, and usually associated with myelomeningocele
- Acquired cerebellar ptosis: Descent of the cerebellar tonsils due to causes other than a small posterior fossa, such as after lumbar puncture or due to intracranial hypotension (pseudotumour cerebri).
Management
- Asymptomatic patients are typically managed conservatively with observation
- Symptomatic patients may require decompressive surgery (suboccipital craniectomy and cervical laminectomy)