Giant cell tumour of bone typically presents in young female adults and is characterised by an eccentrically located, lytic, and expansile lesion in the epimetaphyseal region of long bones, notably around the knee. It is benign with potential for aggressive and rare metastatic potential and is characterised by osteoclast-like giant cells.
Description
Giant cell tumour of bone (GCTB) is a benign, locally aggressive neoplasm that consists of stromal cells and osteoclast-like giant cells. It is most commonly found in the epimetaphyseal region of long bones, predominantly in young adults with a slight female predilection. While benign, its aggressive nature can lead to significant bone destruction and deformity.
Also known as an osteoclastoma.
Pathogenesis
The precise pathogenesis of GCTB is still not fully understood. However, it is believed to originate from the mesenchymal stromal cells that exhibit abnormal proliferation. The resulting tumour contains a mix of these stromal cells and secondary multinucleated giant cells resembling osteoclasts.
Subtypes
No specific subtypes of GCTB have been identified.
Epidemiology, Risk Factors & Associations
- Occurs predominantly in adults aged 20-40 years (peak around third decade).
- Slight female predilection.
- Most common in the epimetaphyseal region of long bones, particularly around the knee.
- Association with Paget’s disease of bone has been reported.
Clinical Features
Typically, patients present with local pain and swelling. A pathological fracture may be the first clinical sign in some cases.
Complications
- Risk of local recurrence post-surgery (~15-50%).
- Rarely, metastasis to the lungs can occur (1 – 6%), likely due to haematogenous spread often after treatment
- Very rarely (<1%), GCTB can undergo malignant transformation typically into a high-grade sarcoma. There is usually a latency period of approximately 10 years. Usually related to radiation therapy of initially benign GCTB.
- Secondary aneurysmal bone cysts may form in up to 14% of cases
Pathological Features
Histopathology
- Macroscopic: The tumour is soft, and the cut surface is greyish-yellow to brown.
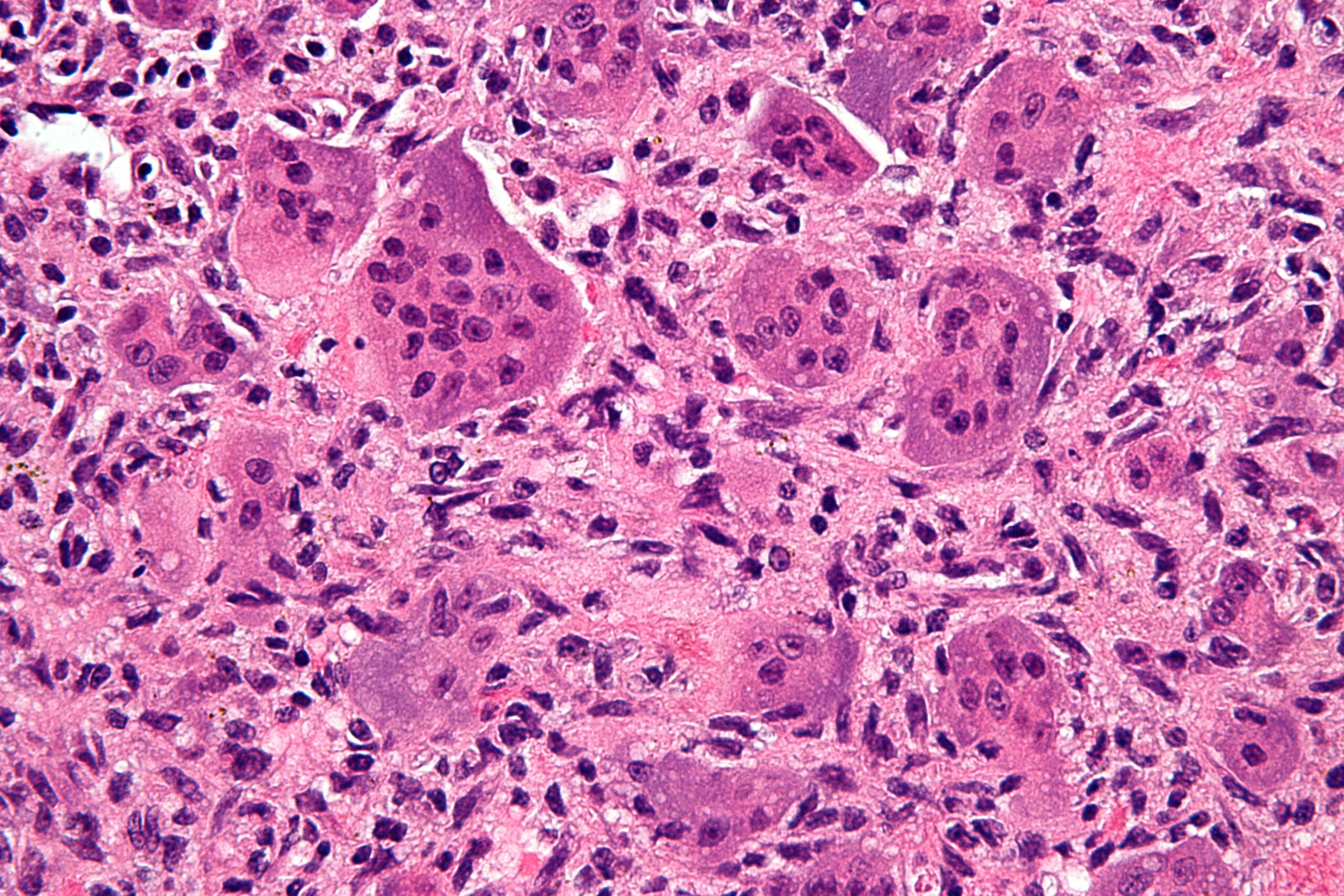
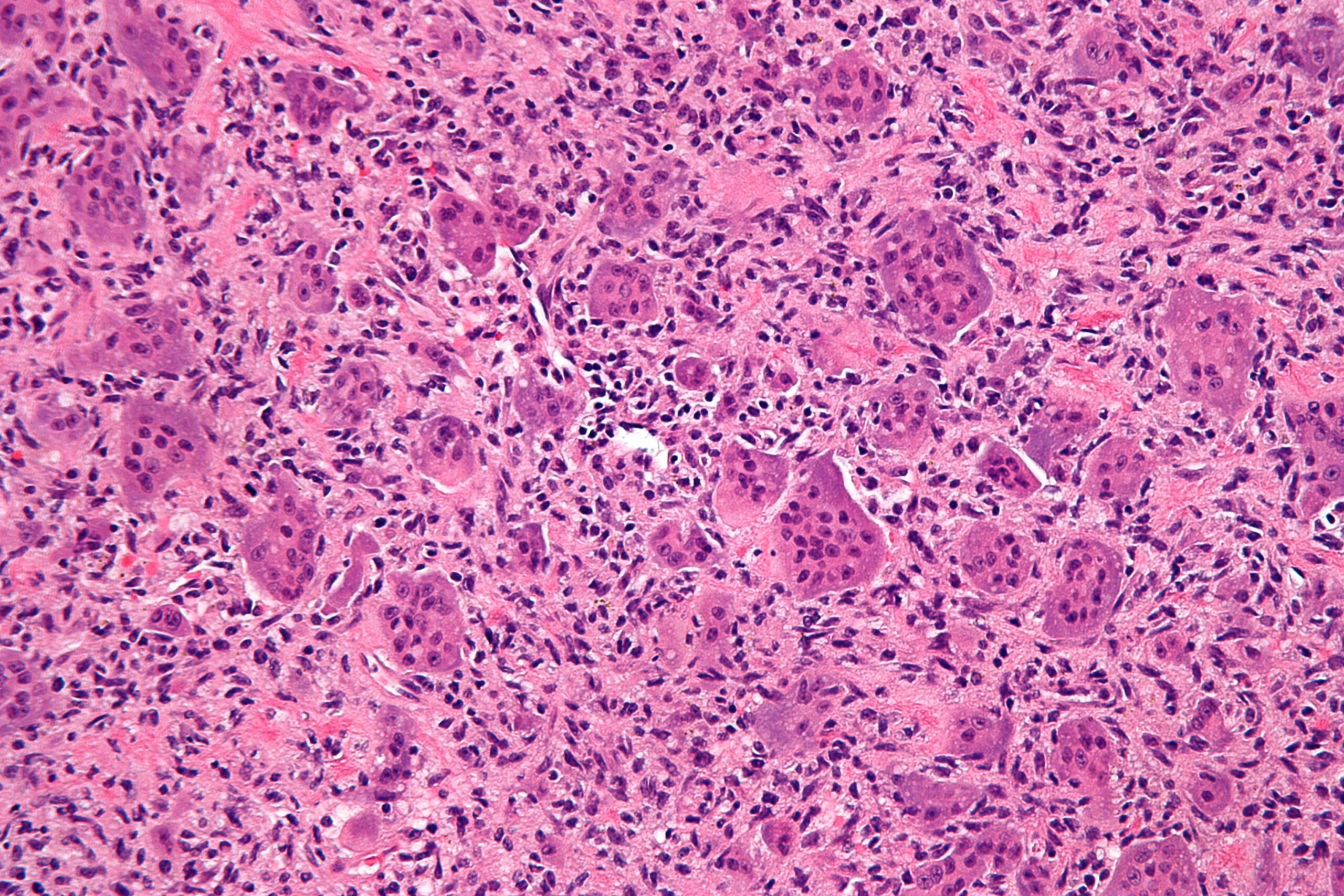
- Microscopic: Characterised by osteoclast-like giant cells dispersed throughout a stroma of mononuclear cells. Haemorrhage and necrosis can be seen. Lung metastases may have a benign pathologic appearance, histologically similar to the primary giant cell tumour.
Serology
No specific serological markers are known for GCTB.
Biochemistry
No specific biochemical markers are known for GCTB.
Radiological Features
General Features
- Characteristically demonstrates an eccentric, lytic, expansile lesion with a narrow zone of transition in the epimetaphyseal region of long bones, extending to the subchondral border (sparing the articular surface)
- Cortical thinning and break-through with soft tissue extension can be seen in aggressive cases.
- No or minimal sclerotic margin.
- Only occurs after physis is closed.
- Rarely multicentric.
- Majority (75-90%) occur in long bones, most commonly the distal femur and proximal tibia, followed by the distal radius. 50-65% occur around the knee.
XR
- Expansile lytic lesion without marginal sclerosis.
- Eccentrically located in the metaphysis and extending to subchondral bone, abuting the articular surface.
- Fused physis
- Cortical thinning
- Geographic with a narrow zone of transition.
- Non-specific periosteal reaction may be seen.
CT
- Non-contrast: Shows detailed bone destruction and cortical breakthrough.
- Contrast-enhanced: Avid heterogenous enhancement.
MRI
MRI findings are nonspecific. A secondary aneurysmal bone cyst may be present.
- T1: Low to intermediate signal intensity. Heterogenous.
- T2/T2 FS: Central regions of low T2 signal is classic. Fluid-fluid levels may be present, but not characteristic. Bone marrow oedema may be present.
- PD FS: Heterogenous hyperintensity. Bone marrow oedema may be present.
- T1 C+: Heterogeneous mild enhancement. Central necrosis may be evident.
- DWI/ADC: Restricted diffusion is not typically seen.
US
- B-mode: Can demonstrate soft tissue extension.
- Colour: Increased vascularity can be seen.
NM
- PET FDG: Uptake is usually moderate to high, correlating with the high cellular activity.
Grading and Staging
Grading of GCTB is not typically performed. Staging is based on the Campanacci system, which describes the extent of tumour aggressiveness and risk of recurrence.
Reporting
Follow-up
Radiographs
- Expect a thin, smooth radiolucent halo around the bone graft or cement following curettage — this represents a normal postoperative interface, not recurrence.
- New or enlarging lytic areas at the graft–host junction or tumour bed should raise suspicion for recurrence.
- Asymmetry, irregular margins, or progressive lucency at prior surgical margins are worrisome features.
MRI
- Methyl methacrylate cement appears dark on all sequences (signal void).
- Recurrent tumour presents as an enhancing, intermediate-signal soft-tissue mass at the cement margin or adjacent bone/soft tissue.
- Use contrast-enhanced MRI for best delineation of recurrence; fat-suppressed T1+C sequences are most sensitive.
- Assess for marrow or soft tissue extension, and evaluate the integrity of the subchondral plate if near an articular surface.
Interpretive Caution
- Differentiate normal postoperative changes (smooth halo, fibrous interface, mild granulation enhancement) from true recurrence (nodular, progressive, enhancing soft-tissue component).
- Correlate with interval change—stability over serial studies supports benign postoperative appearance.
Additional Notes
- Even wide resection does not preclude recurrence; serial imaging remains essential.
- In spinal GCT, radiation therapy may be used where resection is impractical—look for post-radiation marrow signal change, but persistent or enlarging enhancing tissue warrants concern for recurrence or radiation-induced sarcoma.
Diagnosis
Giant cell tumour (GCT) is confirmed by tissue biopsy (often core needle) with histopathological analysis revealing numerous uniformly distributed osteoclast‐like giant cells intermingled with mononuclear stromal cells.
Differential Diagnosis
- Aneurysmal bone cyst: May be secondary to GCTB. Younger patient population, more eccentric location in metadiaphysis, expansile and characteristic fluid-fluid levels on MRI. No solid enhancement. Can be seen in the posterior elements of the vertebra.
- Chondroblastoma: Seen in skeletally immature or young adults. Lytic lesion which originates in the epiphysis rather than metaphysis, sometimes demonstrating chondroid matrix and a much more sclerotic margin. Extensive regional oedema is a differentiating feature.
- Chondrosarcoma: Conventional chondrosarcoma may extend to subchondral bone. Clear cell chondrosarcoma originates in epiphysis. Lobulated high T2 signal is a differentating feature.
- Osteosarcoma: More aggressive radiological features, periosteal reaction, and Codman triangle. Increased age group, with peak incidences in teenagers and the elderly. Telangiectatic osteosarcoma may have the lytic moderately aggressive appearance. MRI would show fluid levels in the majority of this lesion. The recurrence might be expected to be more aggressive in appearance than the one shown here.
Management
Management typically involves surgical resection. Depending on the location and extent of the tumour, this may involve curettage or en-bloc resection. Curetted lesion filled with methyl methacrylate cement or bone graft. In certain cases, pre-operative selective arterial embolisation may be performed. Adjuvant therapies, such as radiation therapy or denosumab, may be considered, especially in cases where complete resection is challenging (e.g. in the spine) or in recurrent disease.