Overview
The sternum (breastbone) is a flat bone, vertically oriented at the midline of the anterior aspect of the thorax. It connects the ribs via costal cartilages and it’s primary function is to protect the underlying mediastinum from injury.
Structure
The sternum is divided into three segments (superior to inferior):

Manubrium
- A trapezoidal-shaped bone, notched at its four borders
- Superiorly: concavity/depression known as the suprasternal notch (jugular notch), visible as a surface landmark.
- Superolaterally: large fossa lined with cartilage known as the clavicular notch, articulates with the medial end of each clavicle to form the sternoclavicular joint
- Inferolaterally: cartilaged lined facet for articulation with the costal cartilage of the 1st pair ribs and a demifacet (half-facet) for articulation with the costal cartilage of the 2nd pair of ribs
- Inferiorly: articulates with the body of the sternum (manubriosternal joint)

Sternal Angle
- The projection formed between the manubrium and sternal body which are vertically oriented in slightly different planes resulting in angulation (also known as the angle of Louis)
- The angle corresponds anteriorly to the intervertebral disc between T4-T5
- The 2nd pair of ribs attach at this junction, palpable as a transverse ridge of bone on the anterior aspect of the sternum and therefore a clinically useful landmark to help number ribs

Body
- Longest part of the sternum
- Flat, elongated bone with depressed facets on the side where costal cartilages of the 3rd to 7th pair of ribs articulate inferior to the sternal angle
- Inferiorly articulates with the xiphoid process (xiphisternal joint)
Xiphoid Process
- Smallest part of the sternum
- A triangular-shaped inferior projection with high variability in size and shape, with its tip located at the level of the T10 vertebrae
- It is mostly cartilaginous until the age of 40 and becomes completely calcified by the age of 60
Arterial Supply
- Horizontal branches of the left and right internal thoracic arteries (also known as the internal mammary artery) – originates from the first part (pre-scalene segment) of the subclavian arteries, namely:
- Sternal branches – main branches supplying the sternum, primarily located in the intercostal space
- Anterior intercostal branches
- Perforating branches
- Non-collateral branches
Venous Drainage
- Internal thoracic vein – drains into the brachiocephalic vein on each side
Muscular Attachments
Manubrium
- Sternocleidomastoid
- Sternohyoid
- Sternothyroid
Body
- Transversus thoracis – also attaches to the xiphoid process
- Pectoralis major
Xiphoid Process
- Diaphragm
- External oblique
- Internal oblique
- Transversus abdominis
- Rectus abdominis
Development
- During the 6th developmental week of fetal life, the sternum develops independently from a pair of sternal bands called “sternal bars” that unite in the midline by the 10th week
- In the 7th week, formation of the primary cartilaginous model of the three sternal segments (manubrium sterni, the body of the sternum and the xiphoid process) occurs
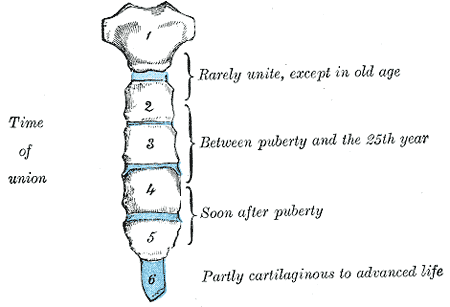
- The cartilaginous sternal model consists of six horizontal divisions known as sternebrae.
- The superior-most sternebra represents the manubrium
- The inferior-most sternebra represents the xiphoid process
- The middle four sternebrae represents the body of the sternum
- The first part of the sternum to form during embryogenesis is the manubrium sterni followed by the sternal body and the xiphoid process.
Variants
- Bifid xiphoid process
- Xiphoid process articulates with part of the costal cartilage of the 7th rib
- Sternal cleft (complete or incomplete) – results form failure of midline fusion of the sternum and can mimic fracture
- Circular shaped sternal formaen – incomplete fusion of the cartilaginous sterrnum
- Pectus excavatum (funnel chest) – inward displacement of sternum and adjacent costal cartilage causing anterior chest wall depression
- Pectus carinatum – outward displacement of sternum and adjacent costal cartilage causing anterior chest wall protrusion (much lower icnidence than pectus excavatum)
- Females have a shorter and thinner body of sternum
- Misplaced sternal angle – can lead to error counting ribs
- Additional sternal symphysis angle – may mimic sternal fracture, traumatic fissure or osteolytic lesion.
References
Anatomy, Thorax, Sternum
https://www.ncbi.nlm.nih.gov/books/NBK541141/
https://www.ncbi.nlm.nih.gov/books/NBK541141/