Overview
The humerus is a long bone of the upper limb, extending from the shoulder to the elbow.
Landmarks
Proximal
- Head – Hemispherical structure projecting anteromedially, articulating with the glenoid cavity, and covered by a layer of hyaline cartilage. On radiographs, its smooth cortical contour should be preserved; irregularity or flattening may suggest degenerative change, osteonecrosis, or fracture impaction.
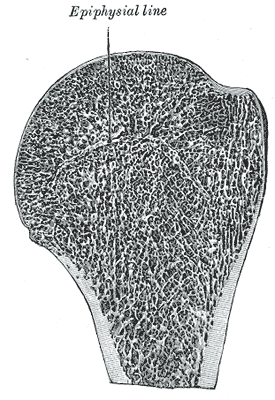
- Anatomical neck – Narrow constriction separating the head from the greater and lesser tubercles laterally, and from the shaft medially. It represents the site of the residual epiphyseal plate. Fractures here are uncommon but carry a risk to the posterior circumflex humeral artery and axillary nerve; on imaging, it appears as a fine cortical line just distal to the articular surface.
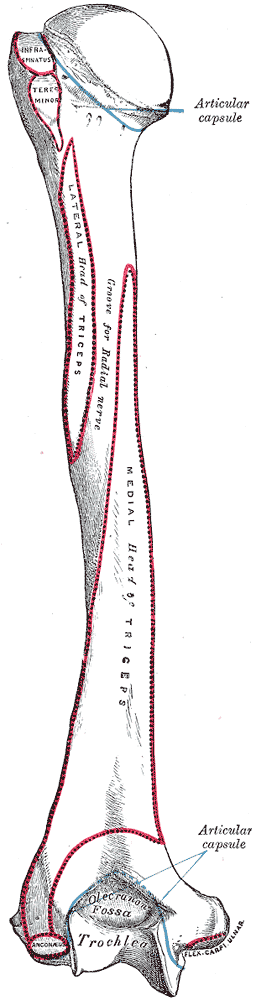
- Greater tuberosity – Prominent lateral projection serving as the attachment site for three of the four rotator cuff tendons: supraspinatus (superior facet), infraspinatus (middle facet), and teres minor (inferior facet). Best visualised with the shoulder externally rotated, where it is projected laterally and free of overlap from the humeral head. In internal rotation, it is superimposed over the humeral head, giving the latter a more rounded profile. Avulsion or impaction fractures of the greater tuberosity are important to detect, as they often accompany anterior shoulder dislocations.
- Lesser tuberosity – Smaller, anteriorly positioned projection on the medial aspect of the proximal humerus, providing the insertion site for the subscapularis tendon (the anterior component of the rotator cuff). Best seen in internal rotation radiographs; in external rotation, it is obscured by the humeral shaft. On axial CT or MRI, it is located anteromedial to the greater tuberosity and forms part of the bicipital groove margin—an important landmark for assessing subscapularis tendon tears and biceps pulley lesions.
- Intertubercular (bicipital) sulcus – Deep groove between the greater and lesser tuberosities, containing the tendon of the long head of the biceps brachii. The groove is lined by a synovial sheath and bridged by the transverse humeral ligament. On MRI, displacement or medial subluxation of the biceps tendon suggests subscapularis injury.
- Lips of the bicipital groove – Margins of the intertubercular sulcus where key muscles insert: the lateral lip receives the pectoralis major tendon, the medial lip receives the teres major tendon, and the floor provides insertion for the latissimus dorsi tendon. These insertional footprints are well demonstrated on high-resolution MRI and are useful landmarks when evaluating tendon avulsions or post-surgical repairs.
| Structure | Muscle / Tendon Attachments | Best Radiographic Projection(s) | Key Imaging Relevance |
|---|---|---|---|
| Head | No direct muscular attachment; articulates with glenoid via hyaline cartilage | AP shoulder (neutral), axial CT/MRI | Assess articular cartilage integrity; look for flattening (AVN), contour disruption (fracture, arthritis) |
| Anatomical Neck | Capsule attachment | AP shoulder (neutral), axial CT | Site of rare fractures; proximity to posterior circumflex humeral artery and axillary nerve |
| Greater Tuberosity | Supraspinatus (superior facet), Infraspinatus (middle facet), Teres minor (inferior facet) | AP external rotation; axial CT/MRI | Fractures often accompany anterior dislocation; insertion site tears on MRI |
| Lesser Tuberosity | Subscapularis tendon | AP internal rotation; axial CT/MRI | Evaluate subscapularis tendon pathology; biceps pulley lesions |
| Intertubercular (Bicipital) Sulcus | Contains tendon of long head of biceps brachii (within synovial sheath) | Axial MRI/CT; ultrasound | Biceps tendon subluxation/dislocation; correlate with subscapularis tear |
| Lips of the Bicipital Groove | Lateral lip: pectoralis major; Medial lip: teres major; Floor: latissimus dorsi | Axial MRI/CT | Tendon avulsion or postoperative tendon reattachment |
| Surgical Neck | No direct tendon attachment; transition to diaphysis | AP shoulder; CT | Common fracture site; risk to axillary nerve and posterior circumflex humeral artery |
| Deltoid Tuberosity | Deltoid muscle | Lateral humerus radiograph | Avulsion injuries, bone marrow oedema in overuse |
| Nutrient Foramen | Vascular entry point for nutrient artery | CT (bone window) | Avoid misinterpretation as fracture |
| Articular Capsule Attachments | Around anatomical neck | MR arthrography | Glenohumeral instability, capsular redundancy or thickening |
Shaft
Cross-section is circular proximally and flattended distally.
- Surgical neck – narrow superior part, immediately below head and tubercles, where axillary nerve and anterior and posterior circumflex humeral vessels lie against
- Deltoid tuberosity – roughned V shaped surface serving as attachment of deltoid on lateral aspect of humerus, anteriorly continuous with lateral lip of bicipital groove
- Radial groove – shallow depression that runs diagonally down the posterior surface of the humerus, parallel to the deltoid tuberosity, contains profundabrachii artery and radial nerve
Distal
- Capitulum – lateral, hemispherical, projects anteriorly, slightly inferiorly. Articulates with the radius.
- Trochlea – medial, pulley-shaped, medial convexity more pronounced (contributes to carrying angle of elbow joint). Articulates with the ulnar.
- Medial and lateral epicondyles – bony protuberances on either side of articular condyles, for attachment of muscles of anterior and posterior compartments of forearm respectively. The medial is larger. The ulnar nerve passes in a groove on the posterior aspect of the epicondyle.
- Radial fossa – anterior depression superior to capitulum
- Coronoid fossa – anterior depression superior to trochlea
- Olecranon fossa – posterior depression superior to trochlear
Articulations
Shoulder (proximally)
- Glenohumeral joint – humeral head articulates with the glenoid fossa of the scapula
Elbow (distally)
- Humeroulnar joint – trochlea of the humerus articulates with trochlear notch of ulnar
- Trochlea is latin for pulley
- Humeroradial joint – capitulum of the humerus articulates with the head of radius

Arterial Supply
Humeral Head
The anterior and posterior circumflex arteries arise from the axillary artery, with each
giving rise to an ascending branch that enters the humerus and flows retrograde (distal to
proximal) into the anatomic head as the arteria arcuata.
Minor contributions arise from the arteries of the rotator cuff via the greater tuberosity and from the intraosseous metaphyseal artery within the humeral shaft.
- Anterior circumflex humeral artery
- Arises from the third part of the axillary artery at the lower border of the subscapularis
- Runs horizontally, beneath the coracobrachialis and short head of the biceps brachii muscle, in front of the neck of the humerus.
- On reaching the intertubercular sulcus, it gives off a branch which ascends in the sulcus to supply the head of the humerus and the shoulder joint.
- The trunk of the vessel is then continued onward beneath the long head of the biceps brachii and the deltoid muscle, and anastomoses with the posterior humeral circumflex artery.
- Smaller than the posterior circumflex humeral artery
- Posterior circumflex humeral artery
- Arises from the third part of the axillary artery at the lower border of the subscapularis
- It runs posteriorly with the axillary nerve through the quadrangular space.
- It winds around the surgical neck of the humerus and is distributed to the deltoid muscle and shoulder-joint, anastomosing with the anterior humeral circumflex and profunda brachii artery
- It supplies the teres major, teres minor, deltoid, and (long head only) triceps muscles
- Profunda brachii (deep artery) artery
- Brachial artery
Development
- As with many of the long bones within the appendicular skeleton, the humerus develops via endochondral ossification (replacement of cartilage template by bone)
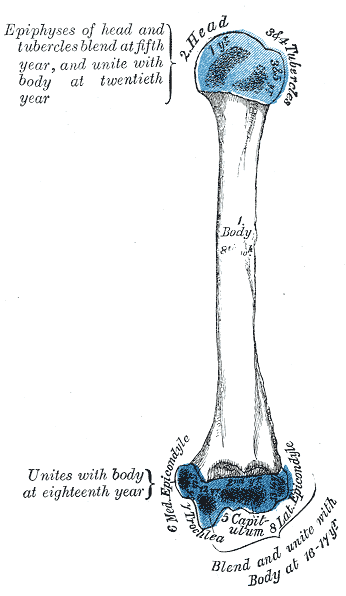
- There are eight humeral ossification centres:
- Head of humerus
- Shaft
- Greater and lesser tubercles
- Medial and lateral epicondyles
- Trochlea
- Olecranon
- The ossification of the shaft occurs at eight weeks gestation, with the humeral head ossification occurring at birth/after birth.
- The greater tubercle’s ossification takes place during the first year of life and the lesser tubercle ossification within the first six years of life.
- By the time of adolescence, all proximal ossification centers of the humerus have fully fused with the shaft.
- The distal ossifications at the condyle and trochlea and olecranon take place between early and later adolescence and fuse with the shaft of the humerus by late adolescence.
References
Anatomy, Shoulder and Upper Limb, Humerus
Evan Mostafa; Onyebuchi Imonugo; Matthew Varacallo.
https://www.ncbi.nlm.nih.gov/books/NBK534821/
Evan Mostafa; Onyebuchi Imonugo; Matthew Varacallo.
https://www.ncbi.nlm.nih.gov/books/NBK534821/