Overview
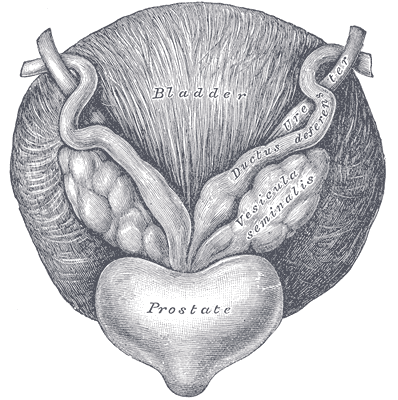
The prostate is a firm, inverted-pyramid-shaped walnut-sized fibromuscular accessory gland in the male reproductive system that surrounds the prostatic urethra and is situated in the true pelvis. It secretes proteolytic enzymes into the semen, which act to break down clotting factors in the ejaculate.
Structure
It has a superior base, inferior apex, and three surfaces (anterior, inferolateral and posterior). Approximately two-thirds of the prostate is glandular in structure and the remaining third is fibromuscular. The prostate gland itself is surrounded by a thin fibrous connective tissue pseudocapsule.
Anatomical Lobes
Traditionally, the prostate is divided into anatomical lobes (anterior and posterior lobes, two lateral lobes, and one median lobel) by the urethra and the ejaculatory ducts as they pass through the organ.
Histological Zones
- Peripheral zone – makes up the main body of the gland (approximately 70%) and is located posteriorly. It surrounds most of the central zone and partially surrounds the distal part of the prostatic urethra
- The ducts of the glands from the peripheral zone vertically empty in the prostatic urethra
- Vertical orientation allows urine reflux which may explain tendency for inflammation in this zone
- Palpapble against the rectum on digital rectal examination
- The ducts of the glands from the peripheral zone vertically empty in the prostatic urethra
- Central zone – surrounds the ejaculatory ducts, comprising approximately 25% of normal prostate volume.
- The ducts of the glands from the central zone obliquely empty into the prostatic urethra, thus being rather immune to urine reflux.
- Transitional zone – located centrally and surrounds the urethra, comprising approximately 5-10% of normal prostate volume.
- The glands of the transitional zone are those that typically undergo benign hyperplasia (BPH)
- Fibromuscular stroma (or fourth zone) is situated anteriorly in the gland. It merges with the tissue of the urogenital diaphragm

Anatomical Capsule and Surgical Capsule of the Prostate
| Feature | Anatomical Capsule | Surgical Capsule |
|---|---|---|
| Definition | True fibromuscular layer surrounding the prostate | A histological boundary between transition zone (TZ) and peripheral zone (PZ) |
| Histology | Dense connective tissue + smooth muscle | Not a true capsule; composed of compressed prostate tissue |
| Anatomical Location | Outermost layer of the prostate | Internal, encircles the transition zone |
| Seen on Imaging? | Rarely visualised clearly on MRI | Often visible on T2-weighted MRI as a hypointense line |
| Clinical Importance | Relevant for staging (e.g. extracapsular extension) | Important in BPH surgery (e.g. TURP plane) |
Surfaces
Anterior Surface
- Forms posterior limit of the retropubic space
- Connected to the pubic bone by the puboprostatic ligaments
Posterior Surface
- Triangular and flat
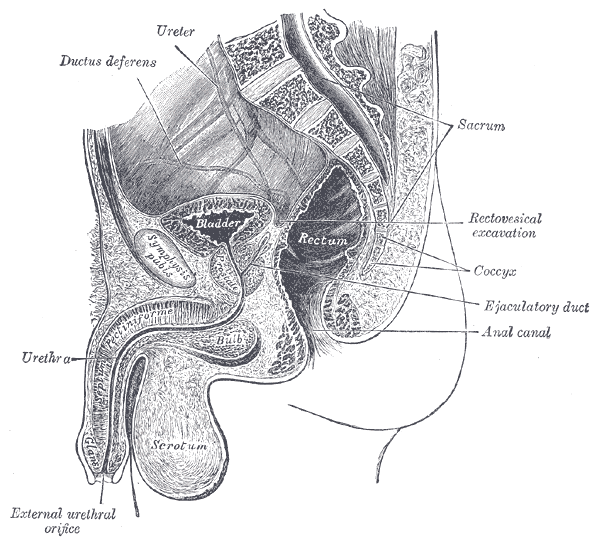
- Anterior to the rectum – separated by the rectovesical fascia
- Vertical median groove
Inferolateral Surface
- Rests on the levator ani fascia
Contents
Proximal Urethra
- Originates in the region of the bladder neck, courses roughly 2.5 cm inferiorly and terminates at the membranous urethra
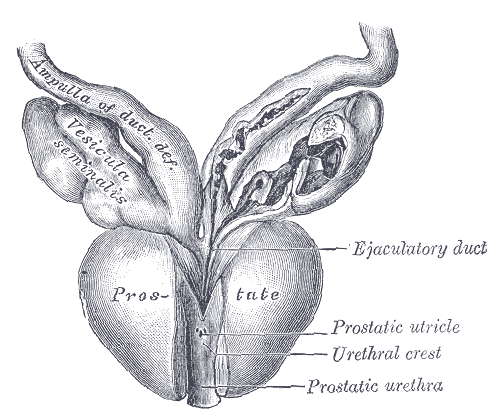
Ejaculatory Ducts
- Paired structures formed by the union of the vas deferens with the duct of the seminal vesicle
- Enters the prostate immediately as it emerges from the seminal vesicles.
- Both ducts travel from posterior and lateral to medial and inferior, converging at the urethra within the prostate gland and opening at an area called the seminal colliculus
Arterial Supply
- Prostatic branch of the inferior vesical artery (anterior division of the internal iliac artery)
- Also contributed to by internal pudendal and middle rectal arteries.
Venous Drainage
- Prostatic venous plexus (Santorini’s plexus) – drains into the internal iliac veins
- Tributaries:
- Pudendal plexus
- Deep dorsal vein of the penis (drains to internal iliac vein)
- Batson’s venous plexus – network of valveless veins that connect deep pelvic veins draining the bladder, prostate, and rectum to the internal vertebral venous plexus, thereby allowing metastatic and infectious spread to the spine
Lymphatic Drainage
- Mainly to obturator and internal iliac nodes
- Some drainage to external iliac, presacral and para-aortic nodes
Innervation
- Prostatic nerve plexus – extension of the inferior hypogastric plexus, supplies sympathetic, parasympathetic and sensory fibres
- Sympathethic (L1 – L2) – The smooth muscle of the prostate gland is innervated by sympathetic fibres, which activate during ejaculation
- Parasympathetic (S2 – S4) – Pelvis splanchnic nerves
Note: The splanchnic nerves are paired, autonomic nerves that carry both visceral sympathetic and sensory fibers, except for the pelvic splanchnic nerves which carry parasympathetic fibers.
Relations
Anterior
- Retropubic space
- Pubic symphysis – separated by retropubic fat and prostatic venous plexus.
Posterior
- Rectum – separated by fascia of Denonvilliers
Superior
- Bladder
- Seminal vesicles (superior-posterior) – ejaculatory ducts pierce the posterior surface of the prostate below the bladder and empty into the prostatic uretra
Inferior
- Urogential diaphragm
- External urethral sphincter muscle – wraps around the urethra help to control ejaculatory and urinary flow
Lateral
- Levator ani muscle of the pelvic floor – covered by endopelvic fascia
- Prostatic venous plexus
Development
- The central zone forms from the Wolffian duct whereas both the transition and peripheral zones arise from the urogenital sinus
- The prostate gland starts to develop laterally as epithelial buds from the urogenital sinus wall. These buds branch into solid cords which canalize and form the ducts and acini.
- The surrounding urogenital sinus mesenchyme forms the interfascicular fibroblasts and the smooth muscle of the prostate
- With androgenic stimulation of the androgen receptor expressed in prostatic Mullerian mesenchyma, the prostate forms
- In development, androgen secretion by Leydig cells is the chief regulator of prostate growth
Imaging Features
CT
- Location: Retrovesical, inferior to the bladder, anterior to the rectum.
- Density: Homogeneous soft tissue density (~30–45 HU), poorly distinguished from surrounding structures.
- Capsule: Not clearly visualised.
- Zonal anatomy: Not appreciable.
- Calcifications: Common in the central gland (especially in older men).
- Use: Limited for primary prostate assessment; mainly for staging (lymphadenopathy, bone metastases, bladder involvement).
US
- Modality: Typically transrectal (TRUS).
- Echotexture:
- Peripheral zone: Hyperechoic or isoechoic
- Transition zone: Variable echogenicity, often more hypoechoic with BPH changes
- Shape: Ovoid, symmetrical
- Capsule: Hyperechoic line outlining the gland
- Median sulcus: Midline indentation, may be visible
- Calcifications: Echogenic foci with posterior acoustic shadowing
- Use: Volume estimation, biopsy guidance, limited cancer detection
MRI
Zonal Anatomy
- Peripheral Zone (PZ):
- Posterolateral
- T2: High signal intensity, homogeneous (due to abundant glandular tissue with high water content from prostatic secretions)
- T1: Intermediate
- DWI/ADC: May show restricted diffusion if tumour present
- Transition Zone (TZ):
- Central anterior region around urethra
- T2: Heterogeneous low/intermediate signal; “organised chaos” due to BPH nodules
- T1: Intermediate
- DWI/ADC: Tumours here may show restricted diffusion but can be hard to differentiate from BPH
- Central Zone (CZ):
- Posterior base surrounding ejaculatory ducts
- T2: Symmetrically low signal, often wedge-shaped
- Important not to confuse with tumour
- Anterior Fibromuscular Stroma:
- T2: Low signal (due to fibrous tissue and muscle)
- Non-glandular, tumour rare
- Surgical Capsule:
- Appears as a hypointense line between TZ and PZ on T2
- Useful for identifying BPH nodules
Other features
- T2 hyperintense signal which surrounds the prostate represents the prostatic venous plexus.
Other MRI Sequences
- T1-weighted:
- Prostate: Intermediate signal
- Highlights haemorrhage (post-biopsy) and proteinaceous material
- Cancer not well seen on T1
- Diffusion-Weighted Imaging (DWI):
- Cancer: High signal on high b-value DWI, low signal on ADC (restricted diffusion)
- Dynamic Contrast Enhancement (DCE):
- Cancer: Early, focal enhancement and washout
- Helps assess PI-RADS 3 lesions in PZ
Clinical Significance
Radical Prostatectomy – It is flanked by the two neurovascular bundles that travel through the pelvic floor towards the penis, supplying it with nerve fibres and blood vessels for the corpora cavernosa. At risk of damage during radical prostatectomy, resulting in erectile dysfunction.
Anatomical Variants
- Absence of the middle lobe