Overview
The liver is a wedge-shaped peritoneal organ located predominantly in the right upper quadrant (right hypochondrium and epigastric) of the abdomen. It is the largest gland in the body, weighing 1.5kg. It is covered by a fibrous layer known as Glisson’s capsule.

Structure
The liver is anatomically divided into left and right lobes by the attachment of the falciform ligament. The right lobe gives rise to two accessory lobes:
- Caudate lobe – located on the upper aspect of the visceral surface, between the inferior vena cava and a fossa produced by the ligamentum venosum (remnant of the foetal ductus venosus)
- Quadrate lobe – located on the lower aspect of the visceral surface, between the the gallbladder and a fossa produced by the ligamentum teres (remnant of the foetal umbilical vein)

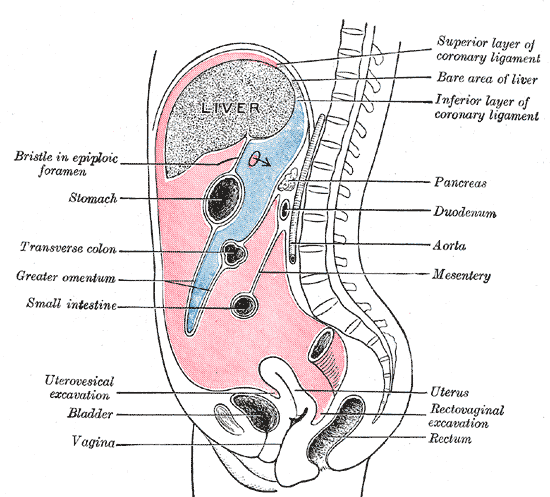
Separating the caudate and quadrate lobe is the porta hepatis, a deep transverse fissure where all vessels (except the hepatic veins), nerves and ducts enter or leave the liver.
Segments
The liver can also be functionally divided using the Couinaud system into eight subsegments, based on a transverse plane through the bifurcation of the main portal vein.
Each segment has its own vascular inflow, outflow and biliary drainage. In the centre of each segment are branches of the portal vein, hepatic artery, and bile duct. In the periphery of each segment is vascular outflow through the hepatic veins.
The classification system uses the vascular supply in the liver to separate the functional units (numbered I to VIII) with unit 1, the caudate lobe, receiving its supply from both the right and the left branches of the portal vein. It contains one or more hepatic veins which drain directly into the inferior vena cava.
The remainder of the units (II to VIII) are numbered in a clockwise fashion.
Surfaces
- Diaphragmatic surface – anterosuperior surface of liver. Smooth and convex, curvature congruent with the under surface of diaphragm.
- Visceral surface – posteroinferior surface of liver. Mostly covered by peritoneum (except fossa of gallbladder and porta hepatis)
A sharp inferior border separates the right and anterior surfaces from visceral surface. It is notched by the ligamentum teres, which lies in the free lower margin of the falciform ligament.
Ligaments
- Falciform ligament – sickle-shaped ligament, attaches the anterior surface of the liver to the anterior abdominal wall, divides the left and right lobes of the liver.
- Ligamentum teres (round ligament) – remnant of the left umbilical vein (connecting the placenta and the umbilical portion of the left portal vein), forms the free border of the falciform ligament
- Coronary ligament – attaches the superior surface of the liver to the inferior surface of the diaphragm, demarcating the bare area of the liver.
- Triangular ligaments:
- Left triangular ligament – attaches the left lobe to the diaphragm. Formed by the union of the anterior and posterior layers of the coronary ligament at the apex of the liver.
- Right triangular ligament – attaches the right lobe to the diaphragm. Formed by union of naterior and posterior layers of the coronary ligament at the apex of the liver
- Ligamentum venosum – fibrous remnant of the ductus venosus of the foetal circulation. Usually, it is attached to the left branch of the portal vein within the porta hepatis. May be continuous with ligamentum teres.
- Lesser omentum – Attaches the liver to the lesser curvature of the stomach and first part of the duodenum. It consists of the:
Hepatic Recesses
Anatomical spaces between the liver and surrounding structures which are of clinical importance as infection may collect in these areas, forming an abscess.
- Subphrenic spaces – located between the diaphragm and the anterior and superior aspects of the liver. They are divided into a right and left by the falciform ligament.
- Subhepatic space – located between the inferior surface of the liver and the transverse colon.
- Morison’s pouch – a potential space between the visceral surface of the liver and the right kidney. This is the deepest part of the peritoneal cavity when supine (lying flat).
Blood Supply
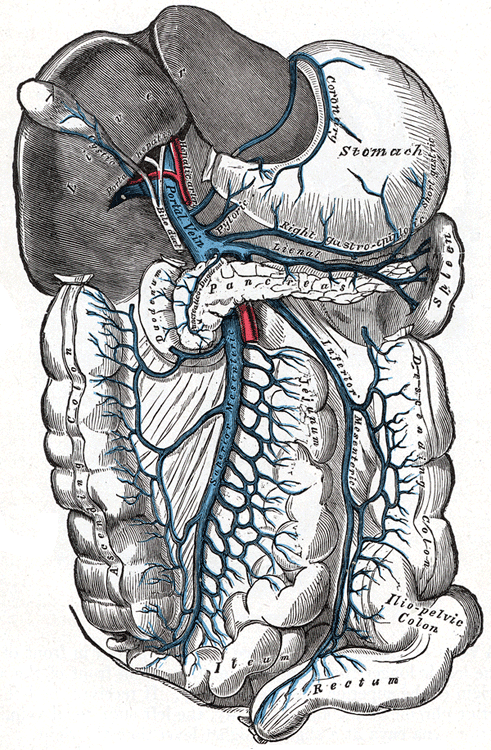
- Portal vein (75%) – supplies partially deoxygenated blood, carrying nutrients absorbed from the small bowel.
- Hepatic artery proper (25%) – supplies non-parenchymal structures of the liver with arterial blood
- The common hepatic artery branches from the coeliac trunk. It gives off the right gastric artery (anastomoses with left gastric artery – another branch of the coeliac trunk), gastroduodenal artery (anastomoses with right gastro-epiploic artery – a branch of the splenic artery), before continuing as the hepatic artery proper which bifurcates to left and right hepatic arteries.
- The hepatic artery proper is part of the portal triad (including the portal vein and common bile duct), which runs in the hepatoduodenal ligament. The hepatoduodenal ligament extends from the superior part of the duodenum to the porta hepatis.
- Right hepatic artery
- Anterior branch supplies segments 5 and 8 (usually supplies a branch to segment 1)
- Posterior branch supplies segments 6 and 7
- Cystic artery within Calot triangle – supplies gallbladder
- Middle hepatic artery
- Middle hepatic artery – supplies segments 4a and 4b (may arise from right hepatic artery)
- Left hepatic artery – supplies segments 2 and 3
Venous Drainage
Three large intrahepatic veins drain the liver parenchyma, into the inferior vena cava:
- Right hepatic vein – runs in the right hepatic fissure and drains segments 5, 6, 7 and 8. The vertical plane of the right hepatic vein separates the segments 6 and 7 (posterior to the plane) from segments 5 and 8 (anterior to this plane).
- Middle hepatic vein – runs at the middle hepatic fissure and drains segments 4a, 4b, 5 and 8. The vertical plane of the middle hepatic vein separates the segments 5 and 8 (posterolateral to this plane) from segments 4a and 4b (anteromedial to this plane).
- Left hepatic vein – runs partially in the fissure for the ligamentum teres and the left hepatic fissure. It drains segments 2, 3, 4a and 4b. It is always located anterior to the left portal vein. The vertical plane of the left hepatic vein separates the segments 4a and 4b from segments 2 and 3.
- Caudate lobe veins – The highly variable caudate lobe veins (or a single vessel) drain directly into the inferior vena cava. These veins are occasionally referred to as the Spigelian veins and may become prominent in the setting of hepatic venous obstruction, as in Budd-Chiari syndrome.
Innervation
- Hepatic plexus – innervates parenchyma. Contains sympathetic (coeliac plexus) and parasympathetic (vagus nerve) nerve fibres which enter at the porta hepatis and follow the course of branches of the hepatic artery and portal vein.
- Branches of lower intercostal nerves – innervates Glisson’s capsule
Lymphatic Drainage
- Anterior aspect of the liver – drain into hepatic lymph nodes. These lie along the hepatic vessels and ducts in the lesser omentum, and empty in the colic lymph nodes which in turn, drain into the cisterna chyli.
- Posterior aspect of the liver – drain into phrenic and posterior mediastinal nodes, which join the right lymphatic and thoracic ducts.

Relations
Posteriorly
- Right kidney (posteromedial)
- Right adrenal gland (posteromedial)
Anteriorly
- Ascending colon
Medially
Laterally
- Intercostal muscles
Superiorly
- Right hemidiaphragm
Variant Anatomy
- Riedels lobe – downward tongue-like projection of the anterior edge of the right lobe
- Beaver’s tail – left lobe extends laterally to contact and enclose the spleen
- Hepatic arterial anatomy variants:
- Right hepatic artery arises from the superior mesenteric artery
- Left hepatic artery arises from the left gastric artery – branch of the coeliac trunk
- The right hepatic vein is a single dominant vein in ~70% of individuals
- Accessory right inferior hepatic vein (commonest variant of the hepatic vein)
- Early bifurcation, early trifurcation or even multiple right hepatic veins entering the inferior vena cava